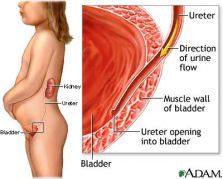
The urologist deals with the surgical diseases of the urinary system of men and women and of the reproductive system of men. Thus he deals with kidney diseases, principally tumours, renal calculi and generally conditions where the outflow of the urine from the drainage system of the kidneys is obstructed. He treats diseases of the ureters, which are most commonly calculi, tumours and obstructions of their orifices within the bladder. He treats diseases of the urinary bladder, which are tumours, inflammations due to bacteria or other factors, some types of urinary incontinence and cacluli. He treats diseases of the prostate, which are prostate cancer and the benign enlargement of the prostate, which can cause urinary hesitancy. He treats diseases of the testicles and their functional parts, such as cryptorchidism, tumours, inflammations and infertility or reproduction disability. He treats penis disorders, such as tumours, the congenital or acquired penile angulation and impotence. He finally treats some special problems, such as urinary incontinence and problems of the urinary tract, which can occur in specific patient groups, such as paraplegic, quadriplegic, diabetic, and parkinsonian patients, etc.
Unfortunately, in many cases, some diseases that can be serious and life- and health- threatening, such as neoplasms, do not present any symptoms before reaching an advanced stage, and thus, it is difficult or even impossible to treat them. On the other hand, some other conditions may present obvious symptoms, without causing serious problems, as in the case of a renal colic, which is due to the passing and elimination of a small stone, of a diameter smaller than 4 millimeters. Therefore, neither should the patient be kept away from the doctor if there are no obvious symptoms, nor is the presence of obvious symptoms a sign of a worrying condition. Having taken these into account, as well as the fact that the symptoms causes are not mentioned, since the purpose of this updating is not the self-diagnosis and self-medication, the most common symptoms in case of which the patient must contact the urologist are:
- Haematuria
- A change in the color and consistency of the urine
- Smelly urine
- Significant reduction or increase of the urine’s quantity
- Deep pain in the kidney area
- Colic (severe pain in the area of the kidneys or the ureters, that usually radiates to the testicle or the labium majorum and is accompanied by vomiting or nausea)
- Pain low in the abdomen, at the height of the urinary bladder
- Pain in the testicles
- Pain in the perineum or in the area of the anus
- Pain during ejaculation
- Pain while the bladder is filling or during urination
- Tingling or burning sensation during urination
- Tingling along the urethra
- Itching with or without the presence of red dots or white coating on the penis glans
- Fluid outflow from the urethra
- Blood or change of color or quantity or consistency of the semen
- Erectile dysfunction
- Ejaculatory disorders
- Inability to conceive after a year of free sexual intercourses
- Swelling in the lower abdomen
- Swelling or palpable mass in the testicles
- Difficulty starting urination or during the entire urination process
- Interrupted urine flow
- Reduction of the urine radius or spreading of the urine flow
- Highly increased urinary frequency
- Severe nocturia
- Sudden need to urinate, which is urgent and peremptory
- Urinary incontinence due to coughing, sneezing, laughing or standing up too fast
- Involuntary loss of urine
- Fever accompanied by pain in the genitourinary system or dysuria or haematuria
Although all urologists are trained to treat all the diseases of the genitourinary system, the scientific progress and the wide range of specialization that exists, as well as the rarity of certain diseases, resulted to the creation of certain subspecializations of urology, in which the urologists are specializing. These are andrology, that deals with infertility and impotence, pediatric urology, that deals with diseases in children, adolescent urology, that deals with problems of pediatric patients when they enter adolescence, and endoscopic urology, that deals with the treatment of diseases, mainly lithiases, with the aid of instruments and telescopes, that are operated within the cavities of the urinary system, in order to avoid large scale surgical procedures. Furthermore, the urogynecology, which deals with the problems of the urinary bladder and of the urethra of women and mainly with the urinary incontinence and the complications of gynecologic surgery, the neurourology, that deals with the urinary problems of patients with neurological disorders, the urologic oncology, that deals with the benign and, principally, with the malignant neoplasms of the genitourinary system, and the urology of kidney transplantation. New subcategories of the above are constantly occurring as science is progressing and the specialization can even reach a level of single disorders, as, for example, prostate cancer.
Most of the lithiasis cases of the urinary system were previously treated by surgery. Today, with the progress of science, the cases of lithiasis that are treated surgically are much fewer than the ones that are treated conservatively. The simplest way to treat lithiasis is the extracorporeal shock wave lithotripsy.
The extracorporeal shock wave lithotripsy is performed with the use of a special device, without anesthesia, and is quite painless. The breaking up of the stones is performed with the aid of shock waves that are generated by the device and are focused on the stone. This method is effective, easy, fast and painless, and has no side effects in practice.
The endoscopic removal with or without fragmentation of the stones is the second type of treatment, which requires anesthesia, but is not accompanied by a surgical incision, and the recovery is fast and smooth. The endoscopic removal may regard ureteral stones and is performed with the use of the same instrument, which is called ureteroscope, and kidney stones, where it is performed with the nephroscope. The ureteroscopic lithotripsy with the use of a laser is very effective in order to fully eliminate ureteral stones, while causing minimal discomfort to the patient.
The nephroscopic access takes place by a puncture on the patient’s body and the passing of the endoscopic instrument through a percutaneous channel, which is created in a directed manner with the aid of ultrasounds and radioscopy. This is followed by lithotripsy, with the use of an endoscopic lithotripter.
Finally, in the cases of multiple or large stones, that previous treatment techniques have failed to treat or when the appropriate technical infrastructure is not available, open surgery is applied. The lithiasis usually manifests itself with a colic that is with a severe pain in the kidneys or along the ureter and sometimes with haematuria or fever.
The presence of fever should worry the patient, because it is a sign of obstruction of the urinary system. It is good that a urine and blood test is performed in order to find possible predisposing factors in all cases of lithiasis. In cases of persisting or relapsing lithiasis or in the cases that the results of simple laboratory test are abnormal, a more extensive metabolic control of the problem must be performed. The medication can help only in special cases, where there are specific metabolic problems, which are responsible for the frequent formation of stones. However, some general principles which can be applied are the reduction of calcium and of uric acid, by reducing the consumption of dairy and of high quantities of meat, the reduction of oxalates, by reducing the consumption of coca cola, tea, coffee, chocolate and of nuts and dried fruits, and the increase of fluid intake in such a degree, that 2 liters of urine are daily produced.

The extracorporeal shock wave lithotripsy is performed with a special device, which generates and focuses shock waves on the stone, causing thus its fragmentation

A modern extracorporeal shock wave lithotripter.

The focusing of shock waves that are generated by a lithotripsy device, on the stone with the aid of acoustic mirrors.

The shock waves reach their target, without causing any damage to the nearby organs, and fragment the stone.

A ureteral stone, as it appears with the use of the special telescope, which is called ureteroscope. The light blue instrument is the fiber of the laser lithotripter.

Percutaneous nephro-lithotripsy with the use of ultrasounds, that are focused on the stone under direct view, or with the aid of the nephroscope.

Nephroscopic lithotripsy of a kidney stone. The telescopic instrument is inserted through the skin and the stone is fragmented using a camera view, with the aid of a special instrument, which is inserted through the nephroscope.
Unfortunately, in the majority of cases, it is possible that the tumours in the genitourinary system do not present specific symptoms or even no symptoms at all. Examples of such cases are prostate cancer, the symptomatology of which may possibly be similar to the one of the benign prostatic hyperplasia or of prostatitis, and kidney cancer, that presents late symptoms, when it is already widespread.
For this reason, the prevention of tumours of the genitourinary system is very important. The only tumour of the genitourinary system that could be prevented with a simple laboratory and clinical examination is prostate cancer. This is very important, if we consider that prostate cancer is the most common type of cancer among men. Thus, all men over the age of 50 or even 45, especially if there exists a family medical history of prostate cancer for male 1st-degree relatives or of breast cancer for females in the family, should visit a urologist once a year and have a digital rectal examination of the prostate and a specific blood test for the prostate specific antigen PSA. A suspected prostate cancer after these two examinations must be confirmed by a prostate biopsy.
For the other types of tumour of the genitourinary system there is a multitude of laboratory examinations, some of which help in their early diagnosis. However, most of them are still experimental and the ones that are clinically applied are not reliable enough to rule out the possibility of a malignancy. Thus, the patient must at least be aware that the presence of blood in the urine, expecially without any pain, requires an immediate examination by a urologist, in order to rule out a possible malignancy. The ultrasonographic evaluation of the genitourinary system, along with a complete urinalysis, are two simple, fast, easy and cheap examinations, which could be performed once a year or once every two years. This control can prevent many serious illnesses. Finally, patients with specific pre-existing medical problems, should undergo a preventive medical control, after the application of a specific treatment, depending on the type of the disease that will be recommended by their urologist, for example, a cystoscopy every 3 months in case of patients that have undergone a transurethral resection of a bladder tumour.
It is important to clarify that the answer to this question depends on the sex and the age of the patient. It is also important to clarify that all medical conditions that present symptoms of urinary tract infection, that is increased urinary frequency and stinging, are not always due to the presence of bacteria in urine. In small children, the presence of frequent urinary tract infections, especially if they are accompanied by fever of if the child is a boy, should make the parent visit a urologist with his child, and particularly a specialized pediatric urologist. A main concern is that the presence of a possible congenital anomaly of the urinary system of the child should be ruled out.
The most common congenital anomaly is the vesicoureteral reflux. In this condition, usually due to the incomplete development of the ureters in the urinary bladder wall, there is a reflux of the urine to the kidneys during the urination phase. This condition is frequently accompanied by urinary tract infections with fever and, if it remains uncontrolled, it can damage or shut down the kidneys of the child.
This condition is usually treated conservatively, with a preventive antibiotic therapy, because it usually disappears as the child grows up. However, some of the cases must be treated surgically depending on certain criteria, of which the principal are the frequently relapsing infections, despite the administration of antibiotics. This must be decided by the pediatric urologist.
Young women often present simple cystitis with local symptoms and more rarely pyelonephritis, that is an infection with fever and pain in the kidneys. The presence of these conditions does not necessarily mean that there exists some predisposing factor. However, the occurence of more than three episodes of cystitis per year or even of one episode of pyelonephritis requires a radiological and a laboratory control, in order to rule out the presence of an underlying cause.
As it has been mentioned, very frequently, no underlying causes are found in this control. In these cases the normal emptying of the urinary bladder must be controlled. Women, who usually retain their urine for psychological reasons, have often a large remaining quantity of urine in their bladder after urination. This remaining quantity may be infected and cause frequent urinary tract infections. If the remaining quantity of urine is considerable, the bladder must be emptied by self-catheterizations, that the woman must perform additionally to her urinations, twice or three times a day.
However, usually even this problem does not exist. In these cases, where there is no problem, the conditions usually regard young or middle-aged sexually active women. These conditions, that are characterised by relapsing episodes of cystitis symptoms, can be accompanied, or not, by positive urine cultures. These conditions are characterised as urethral syndromes. The cause of the urethral syndrome is not known. Its treatment is empiric, with appropriate measures of strengthening of the normal microbiota - which is frequently impaired by the prolonged and frequent use of antibiotics-, hydration, administration of antibiotics in small quantities and for short time periods and, in case of failure of the treatment, with expansion of the urethra and of the bladder. If there is no underlying cause and the bladder is emptied normally without any remaining urine after urination, and the condition still remains, the symptomatic treatment is enough, in combination with the strengthening of the normal microbiota and of the immune system, without any administration of antibiotics. The patient should be reassured and informed that she is not in danger and that she must take antibiotics only if the symptoms of dysuria, presence of fever, or haematuria persist.
Unlike the case of young women, the presence of urinary tract infection with a positive culture in young men is almost always due to the presence of a predesposing factor. This predesposing factor can be more usually a chronic prostatitis, the presence of a stone in some level of the urinary system or the presence of a congenital anomaly, such as the stenosis of the ureteropelvic junction.
For this reason the examination by a urologist is necessary in all cases of occurence even of one single urinary tract infection in a young man. In men of older age, of 55-60 and more, the occurence of frequent urinary tract infections is usually due to the obstruction of the urine outflow due to an enlarged prostate. In these cases a complete control must be performed in order to find out the degree of the urinary obstruction which is due to the prostate. If the obstruction is significant and the urinary tract infections are frequent, a prostatectomy must be performed. Otherwise, the condition can be treated conservatively.
The reflux of urine from the bladder to the kidneys and the ureter can cause hydronephrosis, urinary tract infections and progressive renal damage.
The medical control in order to find out a possible problem, that prevents the conception of a child, must be performed to the couple after a full year of failure to conceive a child despite the free sexual intercourses. A necessary condition is the providing of advisory services to the couple, so that the intercourses lead to the maximum possibility of conception.
If a couple cannot have a child, in 1/3 of the cases the man is responsible, in 1/3 the woman is responsible and in 1/3 both are responsible. Despite the progress of science, 25% of the infertility cases remain unclear.
Therefore, if it is found out that there is a possible problem to conceive a child, the medical control must include both the examination of the woman by a gynecologist, and the examination of the man by an urologist andrologist. The medical control of the man begins with a spermiogram. The spermiogram must be properly performed and evaluated. The presence of a pathological spermiogram does not necessarily mean that the man is responsible for the failure to conceive a child. This happens only in the cases where there is a total absence of sperm in the seminal fluid. In all other cases the possibility that the male factor plays a role in the infertility is as large as the gravity of the disorder that can be observed in the spermiogram. There are 3 basic causes for the presence of abnormal spermiograms:
The 1st and most frequent cause is varicocele. The varicocele is the formation of varices in the veins of the left -usually- testicle, as the varices that can be observed in the leg veins. The formation of these varices is due to the incompetence of venous valves, that allow the flow of blood from the testicles to the renal veins, which is the end point of the spermatic veins, and has as result the reduction both of the number and of the motility of the produced sperm, due to the increase of the temperature of the testicle and of the concentration of toxic substances.
The diagnosis can be easily made by a clinical examination and is verified by a color Doppler of the vas deferens. The varicocele is the most easily treatable infertility condition, because it can be easily treated with a minor, fast and simple surgical operation, during which the internal spermatic vein is tied and cut. The classical high ligation of the spermatic vein is better than the more “modern” methods, as laparoscopic surgery and microsurgery, and the treatment of the condition by vascular embolism, because it is simple, easy, cheap, fast, with a small incision, fast recovery and is always and shall be always effective.
The 2nd cause of an abnormal spermiogram is the abnormal sperm production by the testicle. It is more rarely due to congenital disorders of the testicles and to hereditary diseases and more frequently to hormonal disorders and to acquired testicle damages, such as lesions, and to drugs or toxic substances. A medical history of cryptorchidism, mumps or testicular cancer can be also referred.
The 3d cause is the normal production of sperm, that is however abnormally transferred from the testicle to its outflow in the prostatic urethra. The most frequent damage is due in this case to inflammations of the genital tract, that cause an obstruction to the outflow of the sperm up to the prostatic urethra, from which the sperm finally outflows. In other countries, where the ligation of the vas deferens is used as a means of male contraception, this also consists an important cause in this category.
The two last causes can be distinguished after the performance of specific hormonal tests and more particularly FSH tests. In the cases where the problem lies in the transfer of sperm, the level of obstruction can be determined by a special radiological examination. Usually these conditions can be treated each time with a different degree of success, that depends on the duration of the obstruction, with the aid of a surgical operation. In the cases of obstructive oligospermia or azoospermia, that cannot be surgically treated, as well as in the cases of low sperm production from the testicles, the treatment takes place by in vitro fertilization or intracytoplasmic sperm injection (ICSI).
The last one, which is also the most effective one, consists a modern technological achievement, which is performed with the injection, with the aid of a microscope, of a single sperm, which is collected and selected from the content of an ejaculation, if there is one, or is collected by a testicle biopsy, if there is no ejaculation, directly into an egg, which is collected from the ovaries of the woman with the aid of ultrasounds, after her previous preparation with the administration of hormones, so that many eggs can be produced.
Improtant factors in order to decide to perform the ICSI are the presence of severe -or not- irrepairable damage to the male sperm and the age of the woman. Despite the progress of science, the percentage of success of an ICSI cycle does not exceed 25 to 30%. The financial and psychological cost and possibly the health cost can be significant. For this reason, all efforts of alternative treatment of the problem must be made and the couple should be reassured; on the other hand there must not be a waste of time waiting unnecessarily or following dubious treatments of male infertility, especially if the woman is over 33 years old.

Twins by in vitro fertilization.

The dilatation of the veins that drain the testes is called varicocele and is a cause of infertility.

The varicocele can be palpable or even visible, when it is large.

Anatomy of the genitourinary system. The bilateral epididymal obstruction (16), the obstruction of the vas deferens (15) or of the ejaculatory ducts (11), usually due to inflammations, can cause an obstruction to the sperm outflow (obstructive azoospermia).

During the intracytoplasmic sperm injection is performed, with the aid of a microscope, the injection of a selected single sperm directly into the egg.
Some problems that can occur to the penis and affect the the performance of the sexual intercourse are:
1st Penile curvature. The curvature of the penis can be congenital, or due to injury or the development of a hard plaque on the upper, lateral or lower surface of the penis, which is called Peyronie’s plaque. Peyronie’s disease is a disease of unknown cause, which is characterised by the thickening and hardening and sometimes calcification of a part of the fibrous sheath of the corpora cavernosa. This condition is not a neoplastic condition. Due to the plaque, a curvature and an angulation of the penis is caused during erection, which often causes severe psychological problems, and sometimes even a functional problem regarding the penetration of the penis, when the curvature is greater than 60 degrees. The medication is usually ineffective, and one must know that the disease is spontaneously resolved in 50% of the cases. If the condition remains stable for six months and discomforts the patient, it can be succesfully treated by a surgical operation with excellent results. The most common technique of folding the fibrous sheath of the corpora cavernosa to the opposite side of the damage is effective, but is accompanied by a loss of the functional length of the penis. For this reason are preferred, depending, of course, on the desire of the patient, the techniques of removal or, even better, of incision of the plaque and the placement of an implant in order to cover the gap.
A 2nd condition, which can cause problems during sexual contact, is the pain in the penis during the vaginal penetration. This condition may possibly accompany the curvature of the penis or be related to the absence of vaginal lubrication, and in this case the penetration is also painful for the woman, but it is usually due to the presence of a frenulum breve. This results to the violent pull of the frenulum during penetration which causes pain and often microhemorrhage. The condition can be treated by a simple minor surgical operation for the resection of the frenulum, because the rupture is usually incomplete and the self-healing of the minor wound with a scar tissue causes the worsening of the local pain.
3d Premature ejaculation often consists a problem in the relationship of the couple. It is due to psychological causes and the impression of each man about the nature of premature ejaculation is different. Psychological exercises that can be performed together by the couple, could help resolve the problem, as well as the use of retardant condoms. The local use of ointments, that reduce the sensitivity of the penis glans, can be also helpful. Finally, if the problem persists, the use, for a short period, of drugs that act as serotonin reuptake inhibitors can resolve the problem.
4th Impression of a small penis. Although the penis can be, in some rare conditions, smaller than the normal size in such a degree, that a full sexual intercourse cannot be performed, in the majority of cases this condition is psychological. That is, the person believes that his penis is so small, that he cannot satisfy his sexual partner or that he cannot perform a sexual contact. After the measuring of the penis and the comparison of its size with the use of appropriate tables, the doctor must reassure the patient and, if this cannot be achieved by the urologist, the patient must ask help from a specialized psychiatrist. The only surgical techniques that allow the safe increase of the penis size and are medically acceptable is the resection of the levator, which is located on the dorsal surface of the penile base and which lengthens the penis by 1.5-2 centimeters, and the placement of subcutaneous implants or materials for the increase of the diameter of the penis. The penis stretching devices have doubtful results and their most reliable use is the prevention of loss of length and of shrinkage after surgical operations. Generally, regarding the field of penis size increase, people that find relevant information in documents or electronic material of dubious and often dangerous content and trust it, must pay particular attention and receive the proper information. Proper information must be provided only by a specialized andrologist.

The fibrous Peyronie’s plaque on the white sheath, that surrounds the corpora cavernosa of the penis, “pulls” them on one side, causing thus a curvature.

The premature ejaculation consists a disturbance in the relationship of the couple.
Device that applies tension to the penis, preventing thus its shrinkage after surgical operations to it. This device cannot lengthen a normal penis.
Impotence or, better, erectile dysfunction is a condition that can occur at any age. It is more frequent in older men, however this does not mean that it always happens, as menopause in women. It was believed in the past that the majority of erectile dysfunction cases is due to psychological factors. Today, with the progress of science, it has been found that more than half of the cases are due to organic factors and, as science progresses, more and more causes of erectile dysfunction are identified. The men that have an erectile dysfunction of a psychological type usually have normal erections during the night or in the early hours of the day. However, this is not always the case.
Despite the numerous and different causes, that can cause erectile dysfunction, the problem is treated in a similar way in the vast majority of the cases. Only in few cases, are identified, after special examinations - which are selected depending on the findings in the medical history and the findings of the clinical examination - special causes, which require a different kind of treatment. However, a visit to the urologist and, even better, to a specialized andrologist is necessary, so that these causes can be ruled out and the appropriate treatment is applied.
Urinary incontinence is the involuntary leakage of urine. It is more frequent in women than in men and, although it does not consist a disease that can cause serious damage on that can be threatening to human life or health, is a particularly disturbing condition, which restricts socially the people that are affected by it.
There are two basic categories of urinary incontinence: To the 1st category belongs the incontinence which is caused by coughing, sneezing, laughing or bending. This is called stress urinary incontinence and occurs more frequently in middle-aged women, who have undergone several child deliveries.
This type of urinary incontinence is due to the relaxation of the pelvic floor muscles due to the deliveries and to the lack of estrogenic hormones, which is observed in women after menopause. This relaxation has the result that the anatomical system of the urinary bladder-urethra is not properly supported. This failure to support this system leads to the leakage of urine as pressure is increasing within the abdomen, which does not happen in normal people.
More rarely, the stress urinary incontinence can occur due to the weakness of the external sphincter continence mechanism.
This form is sometimes observed in neurological patients, but it is more frequent after major pelvic surgeries, mainly for prostate cancer in men.
The second type of urinary incontinence is due to sudden spasms of the bladder, that occur against our will and while we are not in the right space or it is not the right time to urinate. This second type of incontinence, which is called urge incontinence, can be due to certain disorders. These disorders can be neurological diseases or disorders of the urinary bladder wall, such as inflammations or tumours. However, in the majority of cases no known cause exists for this type of incontinence and therefore it is called idiopathic. The most common type of incontinence that is observed in women, is a mixed type stress and urge urinary incontinence.
Other more rare types of incontinence is the overflow incontinence, when the urinary bladder is not normally emptied and urine that cannot be eliminated are retained, due to an obstruction or a muscular weakness of the urinary bladder wall, that cannot contract and pushes the urine forward and the incontinence which is due to the continuous contact of the urinary system with the genital tract of the woman.
Although some of these contacts are congenital, the most common one is the vesicovaginal contact which usually consists a gynecological surgery complication. These two last types of incontinence are constant. For the proper treatment of incontinence, it is important to distinguish its type and its cause. If this does not happen, it is possible that the incontinence will not be treated; on the contrary, it could get worse and further problems could occur, that did not previously exist in the patient. Therefore, before any treatment the patient must visit a urologist or, even better, a urologist who is specialized in urinary incontinence.
The treatment of urinary incontinence is not only surgical. For the first type of incontinence, stress urinary incontinence, there are also non surgical types of treatment. These include specific exercises for strengthening the muscles of the pelvis, with or without the aid of simple or special devices or instruments.
The hormone replacement therapy for women after menopause can also be useful. The surgical procedures, that are applied for the treatment of stress urinary incontinence, aim at the support of the anatomical system of the urinary bladder-urethra and at its restoration to its initial status. These procedures include the placement under the urethra, by several ways and techniques, of special bands of tape, that support the urethra when it is moving, due to the increase of pressure within the abdomen, for example by coughing, and thus the leakage of urine is caused.
Today many of these operations are performed with the use of local anesthesia or by a minor procedure without any incision and are very effective.
The placement of an artificial sphincter, in the case of an incontinence type that cannot be treated by other means and is due to the weakness of the sphincter mechanism, consists an absolutely effective and safe method of treatment of a severe incontinence.
The second type of incontinence, the urge incontinence, is mainly treated with drugs. Newer medicines, that have fewer side effects in comparison with oxybutynin, which is an old drug that causes dry mouth, constipation and tachycardia, are added to the therapeutic arsenal of the urologist. New technological achievements are continuously added to the treatments of urge incompetence, as the neurostimulation of certain roots of the spinal cord with the bloddless placement of special electrodes, that are activated by a pacemaker, which is implanted in the body.
Particularly important is the injection, in the urinary bladder, of botulinum toxin Α, a medicine that reduces the hypercontraction of the bladder and stops incontinence. This injection is performed on a non-hospital basis with the use of local anesthesia, and stops the incontinence of the patient without any of the side effects of the orally administered medication. Its duration is six months and it can be repeated thereafter.
The conditions that cannot be treated by drugs and the conditions where, along with the incontinence there is a urine reflux to the kidneys and high pressures within the urinary bladder, which usually occur in neurological diseases, must be surgically treated. The operation that is usually selected is the augmentation cystoplasty and is performed by placing a section of tubularized small intestine in the bladder, increasing thus its capacity.

Sneezing and coughing cause a significant increase of the intra-abdominal pressure, resulting to the involuntary loss of urine (stress urinary incontinence).
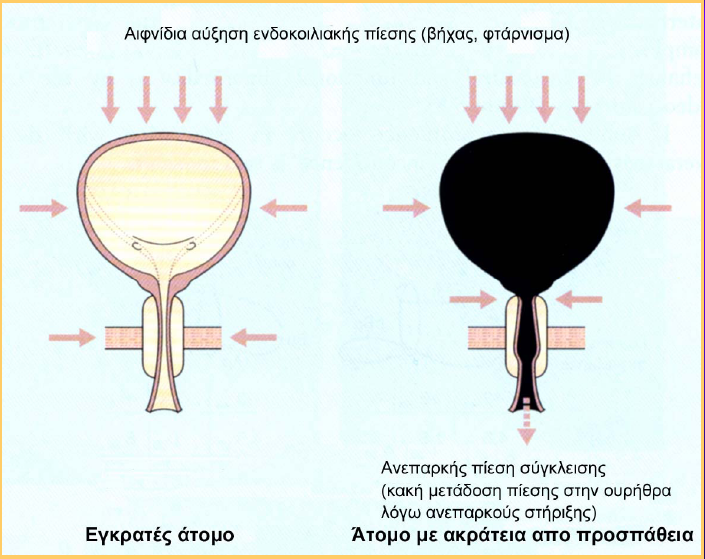
Pathogenic mechanism of the stress urinary incontinence.

Due to the lowering of the bladder and of the urethra during the increase of the intra-abdominal pressure, this high pressure is not transferred to the urethra sphincter, as is normally the case, in order to close it and prevent the leakage of urine, but, on the contrary, it is transferred to the bladder, which in addition to the incomplete convergence of the urethra, acts as a “pipette filler”, intensifying thus the leakage.
 The three types of urinary incompetence. From left to right: a) incontinence due to overflow, caused by an obstruction of the outflow of urine that has not been treated, or caused by a prostate enlargement that has been neglected, b) stress urinary incontinence, c) urge incontinence due to hypercontractivity of the badder muscle due to neurological or other causes.
The three types of urinary incompetence. From left to right: a) incontinence due to overflow, caused by an obstruction of the outflow of urine that has not been treated, or caused by a prostate enlargement that has been neglected, b) stress urinary incontinence, c) urge incontinence due to hypercontractivity of the badder muscle due to neurological or other causes.
Exercises for the strengthening of the pelvic floor, aiming at the improvement of incontinence problems.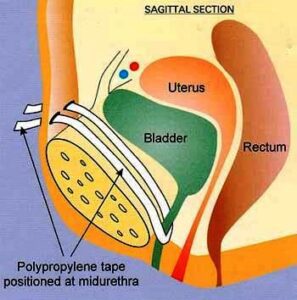
The tension-free tape, which is placed with a simple operation under the urethra, prevents the lowering of the urethra during the increase of the intra-abdominal pressure preventing thus the stress urinary incontinence.
The stimulation of the spinal cord nerves with the use of electric current, which is generated by an electrical stimulator, that is permanently implanted in the body, regulates their function, treating thus the urge incontinence which is due to neurological or unknown causes and activating the contraction of the bladder, so that its emptying is achieved in cases of weakness of the bladder.
 Injection of the botulinum toxin in the bladder.
Injection of the botulinum toxin in the bladder.
 The sites of injection of the botulinum toxin in the bladder for the treatment of urge incontinence.
The sites of injection of the botulinum toxin in the bladder for the treatment of urge incontinence.
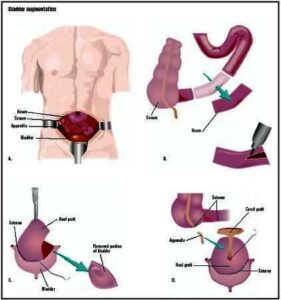 Surgical operation for the increase of the capacity of the bladder and treatment of incontinence by placing a “patch” of intenstine in the bladder, which acts as a “shock absorber”, after the failure of all other treatment methods.
Surgical operation for the increase of the capacity of the bladder and treatment of incontinence by placing a “patch” of intenstine in the bladder, which acts as a “shock absorber”, after the failure of all other treatment methods.
PSA is a relatively reliable index regarding prostate cancer. However, its increase above normal values is not necessarily due to the presence of prostate cancer. There are other conditions that can cause a PSA level increase, unless this has a particularly high value. However, the increase of this index above normal values consists an indication for the control for prostate cancer. The best way to verify the presence of prostate cancer is to perform biopsies, that are directed with the aid of a special ultrasound probe which is inserted rectally.
In the case that the diagnosis of prostate cancer is verified, the staging of the disease follows, that is, determining the extent of the disease, both locally, and in the entire organism in the form of metastases. This is achieved with special examinations. If the disease is limited only in the prostate, the appropriate treatment is the radical prostatectomy or the radiotherapy externally, or by implanting special radioactive seeds in the prostate (brachytherapy), that radiate directly in the gland. Radical prostatectomy seems to be the most appropriate treatment method for younger people, because it secures the elimination of the disease from the human organism and ensures a long-term survival, without the presence of the disease.
Brachytherapy, on the other hand, is gaining ground since it is a minimally invasive technique, with satisfactory results, however it is not free of side effects. If the disease is dispersed throughout the entire body, it is not treatable for the time being, and it is dealt with the aid of hormone medicines, that improve the quality of life and possibly prolong it. If the biopsy is negative, the patient is monotitored through the frequent examination of his PSA. If the PSA shows an increasing trend during this monitoring, the prostate biopsy is repeated once or more times and it is very possible that in one of this repeated biopsies the presence of prostate cancer is discovered. Unfortunately there is no safe method so that the presence of prostate cancer is ruled out in these cases.
The conditions that are related to the enlargement of the prostate are distinguished into two major categories: the prostate cancer and the benign prostatic hyperplasia. The patient who visits the urologist, either for a preventive examination of the prostate, or because he has certain symptoms of irritation or urinary hesitation - the so called symptoms of the lower urinary system -, must undergo 4 simple examinations:
1st The digital rectal examination of the prostate. With this examination is partially evaluated the degree of enlargement of the prostate, but principally the constitution of the gland, which is necessary for the further diagnostic control, in order to verify the existence of a possible prostate malignancy.
2nd An ultrasound of the urinary tract before and after urination. It is necessary to measure the rest of the urine, that remains in the urinary bladder after urination.
3d The measurement of the urine flow. This examination is performed with the use of a special instrument, the uroflowmeter, in order to determine the “intensity” of urination.
4th The measurement of the prostate specific antigen PSA and, when necessary, the determination of the ratio of free prostate specific antigen in total prostate specific antigen.
With the aid of these 4 examinations, the suspicion of prostate cancer can be verified or the presence of prostate cancer can be largely ruled out. In the first case, where there is a suspicion of possible prostate cancer, a prostate biopsy follows, which can verify the presence of the disease. In the second case, where there is no suspicion of cancer, can be -at least roughly- evaluated, with the aid of the first 3 of the 4 aforementioned examinations, the degree of obstruction to the urine outflow that is caused by the enlarged prostate.
In the cases where the patient presents an obstruction of a significant degree, as is evaluated by uroflowmetry, or has presented renal failure, renal dilatation, bladder lithiasis, relapsing urinary tract infections accompanied by fever, persisting haematuria that is not due to some other cause, or complete obstruction of the urine outflow, the surgical removal of the prostate is recommended. In the rest of the cases, where the obstruction degree is not high, the patient’s symptoms are evaluated. If the symptoms are not disturbing the patient, he can be just put under monitoring, and be examined by his urologist once a year. If the symptoms are moderate or severe, the administration of medicines can be tried. If the medication fails to treat the patient and he cannot tolerate his symptoms, a surgical operation is recommended. There are 2 techniques of surgical treatment for benign prostatic hyperplasia. The open prostatectomy and the transurethral prostatectomy.
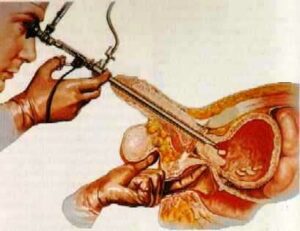
The open prostatectomy is performed with an incision in the lower section of the abdomen, while the transurethral prostatectomy is performed with the aid of a special instrument, that passes through the urethra and removes the prostate, by cutting it into small pieces, that are pulled out through the lumen of the instrument. These two techniques are equally effective. The transurethral prostatectomy has more advantages, due to the shorter hospitalization time of 3 days compared to the 7 days that are required for the open prostatectomy and to its easier postoperative recovery. Neither of the two techniques causes incontinence or impotence. The choice of one of the two techniques depends on the size of the prostate and the existence or non-existence of large stones in the bladder. Thus, in case the prostate is very large or if there are large stones in the bladder, the open prostatectomy is selected, and for smaller stones the transurethral prostatectomy is preferred.
The enlargement of the prostate, under the urinary bladder, causes pressure on the urethra and a urethral stricture, as the urethra passes through the gland, causing thus a urinary hesitancy and a urinary retention, which leads, in the long term, to serious complications and eventually to hydronephrosis and renal damage.
The obstruction of the urine outflow causes guttate urination.

The digital rectal examination of the prostate must be always performed during the urological examination; through this examination can be evaluated the enlargement, sensitivity and induration of the gland, which can be observed in case of benign hyperplasia, prostatitis and prostate cancer respectively.

Uroflowmetry diagram that shows a normal urination. In case of obstruction of the urine due to prostatic hyperplasia or urethral stricture, the curve is more flat and more prolonged.

Uroflowmetry instrument.

Collection of blood for the evaluation of PSA.
Results of prostatic hyperplasia.
