 Although, penis enlargement is a very common reason especially for young men to visit urologist-andrologist, and even a more common reason for searcing the Internet, the truth on a medical basis is that penile size is not an important factor for female orgasm, given the fact that 90% of the sensory nerve terminals, that trigger the sense of pleasure and the contractions of the muscles of the female perineum, which actually represent an orgasm, are located on the clitoris and in the first one centimetre of the vagina. Thus, even a 5cm long penis in erection can be fully sexually functional.
Although, penis enlargement is a very common reason especially for young men to visit urologist-andrologist, and even a more common reason for searcing the Internet, the truth on a medical basis is that penile size is not an important factor for female orgasm, given the fact that 90% of the sensory nerve terminals, that trigger the sense of pleasure and the contractions of the muscles of the female perineum, which actually represent an orgasm, are located on the clitoris and in the first one centimetre of the vagina. Thus, even a 5cm long penis in erection can be fully sexually functional.
In fact, although many men are seeking medical help to get their penis longer and thicker, they really do not have any anatomical or functional problems. Generally speaking most of men, if asked, would wish they had a bigger penis, although at the same time they will admit that they have a satisfactory sexual life. However, some men present a psychological disorder that makes them have a negative view for the size of their penis. This disorder is called “penile dysmorphophobia” and is very stressing.
The condition may regard the size of their penis in the relaxed phase and it is then called “aesthetic dysmorphophobia”, or in the phase of erection and then it is called “functional dysmorphophobia”.Although it looks a bit strange, aesthetic dysmorphophobia is more frequent than functional dysmorphophobia. The disorder can be caused by one more psychologically traumatic events, such as the rejection of the man by one or more sexual companions due to the penis size, or there can be no obvious initial cause in the patient’s medical history.
Patients with this psychological disorder have frequently serious problems to create sexual relationships, due to shame and lack of self-confidence. Sometimes these negative feelings may cause even erectile dysfunction. On the contrary, patients with anatomical micropenis, which is a very rare condition compared to dysmorphophobia, may have a positive view for their personal image and a satisfactory sexual life. Apart from the poor sexual life, dysmorphophobics have an even more serious problem.
Their condition is very persistent and most of the times they do not accept the recommendation of the andrologist to seek psychiatric help. However, even if they do, their problem more frequently will not be solved. Thus, these people are ready to undergo any kind of medication or surgical “therapy” is proposed to them, or they find out on the Internet.
This makes them particularly vulnerable to penis enlargement “treatments”, which may in the best case be ineffective and in the worst dangerous. People that seek such solutions must particularly have in mind, that there is no quality control of the information unlimitedly provided on the Internet and therefore the effectiveness and mainly the safety of the proposed methods are not checked. The truth about the usually presented on the Internet pharmaceutical methods for penis enlargement, is that they do not really exist. That means, that they are completely ineffective and some times cause severe side effects.Also the use of devices, to stretch the relaxed penis for some hours daily, has not been proven to offer remarkable results.
These devices are really useful, after penis surgical operations for various reasons including the enlargement operations or the penile straightening operations in case of Peyronie’s disease. In these cases the postoperative occasional application of stretching for some months can eliminate the shrinkage, which occurs during healing procces of the surgical wound,restoring thus the initial length of the penis.
Surgery can increase both the length and the width of the penis. Many and various techniques are described, both in scientific articles, and on the Internet. Some of them are experimental and some could be also dangerous. The only scientifically documented, safe and acceptable technique for penis enlargement do not, in fact, add centimetres to the penis, but rather try to “dig out” a part of the already existing organ from the surrounding tissues. The operation is performed with general anaesthesia and its duration is 2-3 hours, depending on how many of the following stages will take place.
These stages are:
- Liposuction of the suprapubic area. It is easy and safe and it unburies a part of the penis from the surrounding fat. The more fat exists in the suprapubic region, the better the result.
- Resection of the levator of the penis. This levator is responsible for the upward inclination of the erect penis. Its resection “detaches” a section of the back of the penis, which is located within the body, from the pelvis bone and thus, the penis is mobilised and acquires some additional length. In order to avoid a symphysis reattachment, we place a small lipodermal implant between the bone and the back of the penis. This implant is taken by the region of the patient’s thigh and because it is his body part, we avoid complications that could possibly occur from the use of foreign materials. This procedure is safe. Sometimes, a minor instability of the erect penis is reported, however this does not cause problems.
- Performance of plastic surgery in order to relax the skin on the dorsal surface of the penis and attach the subcutaneous tissue to the periosteum of the pubic bone. It is thus secured, that there is no “pulling” or limitation of the penis mobilisation by the suprapubic skin, and also the effective “unburying” of the penis
- Performance of plastic surgery in order to relax the skin on the ventral surface of the penis, aiming to “transform” a part of the scrotum skin to penile skin. Thus, a part of the ventral surface of the penis is getting free from the scrotum. This step is not always necessary and is not performed, when a simultaneous lengthening and thickening of the penis has been selected.
- The application of stretching to the penis by using a special stretching device. This is applied eight weeks after the operation and for 3-6 months. The aim is to get back the all the obtained by our surgery additional centimetres of the penis length, which are possibly lost, due to postoperative shrinkage caused by the healing process.
- Increase of penis thickness. This can be achieved by two techniques:
a) By placing an implant acting as a “thick sheath” under the skin of the penis and attach it on the base of the penis. This implant can be obtained by the patient’s body and be a “lipodermal” implant taken from the buttocks or the belly. Alternatively an allogeneic implant can be used like pig collagen. The thickness of the implant is added to the diameter of the penis and, thus the overall diameter increases. This technique can be performed simultaneously with penis lengthening. Rare complications can be a partial or total necrosis of penile skin, or fibrosis and shrinkage of the implant. A “foreign” implant, on the other hand, could be infected with devastating results.
b)By the injection by special syringes, of various thick liquid materials under the skin of the penis. These materials can be fat coming from the liposuction of the suprapubic region during the first step of lengthening or hyaluronic acid. The use of liquid silicone, paraffin or other unknown materials can cause serious reactions in the skin of the penis, with devastating consequences and must be avoided. Patient’s fat after a proper processing and centrifugation is placed under the penis skin and is “molded” by the surgeon’s hands, so that it can be evenly distributed under the entire penis surface.
The penis is maintained stretched during the whole procedure, in order to achieve a uniform thickening result during the erection also. Use of patient’s fat helps avoiding complications that may be caused by foreign materials. Sometimes, if the patient wishes, the fat injection can be repeated after 6 months with local anaesthesia.The procedure of thickening of the penis can be performed without a simultaneous lengthening by local anaesthesia only.
 Penile prothesis – The spontaneous solution Erectile dysfunction is the inability to achieve and maintain an erection hard enough to have a satisfactory sexual intercourse in the last six months.In the international study of Massachusetts USA, that consists globally the principal study regarding the evaluation of sexual dysfunction during aging, is mentioned that, in the group of men aged 40-70 years the incidence of complete impotence amounts from 5.1% at the age of 40 to 15% at the age of 70, while the incidence of moderate dysfunction is 17% at the age of 40 and is doubled to 34% at the age of 70.
Penile prothesis – The spontaneous solution Erectile dysfunction is the inability to achieve and maintain an erection hard enough to have a satisfactory sexual intercourse in the last six months.In the international study of Massachusetts USA, that consists globally the principal study regarding the evaluation of sexual dysfunction during aging, is mentioned that, in the group of men aged 40-70 years the incidence of complete impotence amounts from 5.1% at the age of 40 to 15% at the age of 70, while the incidence of moderate dysfunction is 17% at the age of 40 and is doubled to 34% at the age of 70.
In Greece it is estimated that approximately 450,000 men have a moderate degree of erectile dysfunction. Of them, 11,500 men will deteriorate to complete impotence every year. However, the problem is usually not mentioned to the andrologists, mainly due to reasons of shame. Thus, it worsens over time and it is finally leads to depression and social isolation.
Erectile dysfunction can be purely psychological or it may have an organic origin, on which psychological factors are also added, as its appearance causes major stress in every upcoming sexual attempt, leading to repeated cycles of failure to achieve and/or maintain hard erection. In older men the causes are usually multifactorial and can include diabetes, cardiovascular diseases, surgical operations for prostate, bladder or sigmoid cancer, neurological diseases, medicines mainly psychotropics and medicines for heart diseases especially antihypertensive and finally hormonal disorders. In the younger people the causes are mostly psychological factors and chronic prostatitis.
The diagnosis of the cause of the disorder can be made by the andrologist. However, the special causal treatment is usually not possible, except some cases of prostate diseases and hormonal disorders. Fortunately there are ways of non special treatments, which can resolve the problem.
These include:
Orally administered drugs, which improve the blood circulation in the penis and after sexual stimulation they help a week erection to be harder, more prolonged and easier to be achieved. They are generally safe and easy to be used. However, they are not effective in 30% of the cases, particularly in patients with neurological damages, severe vascular diseases and those, who underwent radical prostatectomy. Furthermore, their use is contraindicated in some cases of coronary heart diseases and their frequent use is quite expensive.
The injection of drugs in the corpora cavernosa of the penis produces a hard erection in the most of the patients, even without sexual stimulation. This treatment is more effective than the peels and the drugs act only locally, thus avoiding systemic side effects. However, there can be severe pain, hematomas and hardening of the corpora cavernosa, due to fibrosis in the injection site. Also priapism (prolonged and painful erection) may appear in some cases, which need urgent hospital admission. Furthermore, patients do not feel comfortable with penile self injections and the effectiveness of the treatment is reduced over time.
The placement of a penile prosthesis consists surgically the most effective, permanent and safe treatment for patients, who do not respond to medications, or when there are serious side effects, or when the patients do not wish peels or self injections. Penile prosthesis is a hydraulic implant, which is placed by a relatively simple operation under general or spinal anaesthesia, lasting usually one hour and with one day hospitalization. The incision is small and invisible on the lower ventral surface of the penis and the material is not perceivable even by the patient’s companion during the intercourse.
A recent clinical study presented that the placement of penile prostheses resulted to a much higher satisfaction of men (93%), in comparison with drugs (51%) and injections in the penis (40%). Furthermore, a clinical study in 90 of my personal cases, which has been published in the reputable scientific journal “The journal of sexual medicine”,has shown that there is a full correlation between the sexual satisfaction of the patient after the placement of the prothesis and the sexual satisfaction of his companion.
The superiority of the penile prosthesis is related to the fact that it is the only treatment that allows spontaneous sexual intercourse at any time, as the erection is achieved within seconds without the need of a “preparation” or the possibility of failure (as in the case of peels and injections), and the erection is maintained for as long as the man desires. Furthermore, the sensation, the ejaculation and the orgasm are completely natural as would be without any intervention.
The penile prosthesis consists of three parts. The two cylinders, which are implanted in the corpora cavernosa, which are the two erectile units of the penis, the pump, which is placed within the scrotum and the reservoir, which is placed on the lateral side of the urinary bladder. All these parts are placed into position through a small incision, which is performed on the lower ventral surface of the penis, where the scrotum begins.
Nothing is externally visible and only the pump is palpable by the patient in his scrotum. The function of the prosthesis is purely hydraulic. In order to fill the cylinders with the normal saline existing in the reservoir, thus to inflate the cylinders and achieve a hard erection, is only enough to pump up the lower round part of the pump in a way similar to the inflation of a sphygmomanometer. The erection which is achieved is very hard, the orgasm, the pleasure and the ejaculation are normal, and similar to the sexual intercourse without the aid of the device.
The prosthesis can be deactivated, only when the patient wishes so. This is accomplished by pressing and holding the upper part of the pump, resulting to the return of the saline from the cylinders in to the reservoir and the relaxation of the penis.
The operation is always effective and safe and offers to the patient the possibility to fully recover his lost sexual activity. The implant is never rejected by the human organism. Its lifetime is unlimited, but if there is a mechanical failure, it can be immediately replaced, in the same way it was initially placed, since it has a lifetime guarantee by the providing company. In the very rare case of an implant infection, which is high unlikely, as its surface is covered by an antibiotic film, we remove it and replace it with by a new implant four to five later. Thus, problems from the operation do practically not exist and it is certain that the benefits are outweighing them.
Penile curvature – A frequent tormenting problem
 With the term curvature of the penis we mean the “bending” that may possibly exist on the body of the penis from birth, and in this case it is called congenital curvature, or the one that occurs later in the adulthood, and in this case is called acquired curvature. The curvature can exist in any direction upwards, downwards, to the left or to the right. Usually combinations of the aforementioned curvatures may exist. The curvature can also regard the front half or the rear half of the body of the penis. Finally, the curvature can be small or big, and in this case it can reach or even exceed 90 degrees, making the vaginal penetration difficult or impossible. More rarely, there can be a ring like stenosis somewhere on the body of the penis, and in this case the erect penis has the form of a sandglass.
With the term curvature of the penis we mean the “bending” that may possibly exist on the body of the penis from birth, and in this case it is called congenital curvature, or the one that occurs later in the adulthood, and in this case is called acquired curvature. The curvature can exist in any direction upwards, downwards, to the left or to the right. Usually combinations of the aforementioned curvatures may exist. The curvature can also regard the front half or the rear half of the body of the penis. Finally, the curvature can be small or big, and in this case it can reach or even exceed 90 degrees, making the vaginal penetration difficult or impossible. More rarely, there can be a ring like stenosis somewhere on the body of the penis, and in this case the erect penis has the form of a sandglass.

The congenital curvature can be due to fibrous chords that are located under the skin of the body of the penis. This condition can present alone or usually may accompany a lower position of the urethral meatus on the glance or on the body of the penis. This situation is called hypospadias. More rarely, there can be a disproportion of the length of the corpora cavernosa, which are the basic erectile units of the penis. In this case the penis bends towards the shortest corpus cavernosum.
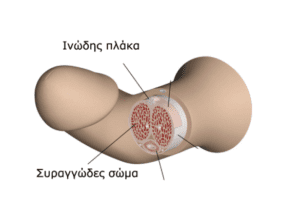
The acquired curvature is due to thickening and hardening of a part of the fibrous sheath, which covers externally the corpora cavernosa, resulting to the formation of a hard fibrous plaque, of a different size in each case, which can easily be palpated. This condition is called Peyronie’s disease, from the name of the French doctor who discovered it and the plaque is called Peyronie’s plaque. This disease has an unknown cause. Sometimes an over bending injury with or without fracture of the erected penis during sex is mentioned, but mostly the medical history is clean. This condition is not cancer.
The hard plaque pulls back during erection and does not allow the proper dilatation and stretching of the corpora cavernosa consequently leading in bending and angulation of the penis. The extent of the curvature depends on the size and the position of the plaque. The Peyronie’s plaque in its initial appearance can be accompanied by painful erection, which is an indication of inflammation in the acute phase of the disease. Over time the pain goes away and only the curvature remains. The acute phase of the disease, which is characterised by the appearance and augmentation of the plaque, can last up to 6 months. After this period the plaque and consequently the curvature are usually stabilized. In 10% of the cases the plaque may resolve and the penis may become straight again without treatment.
Penile curvatures often causes severe psychological problems, and sometimes in cases of curvatures bigger than 30 degrees functional problems during vaginal penetration may appear. In these cases patients have to straighten their penis by holding it to achieve penetration and they also have to avoid specific positions during sex. Pain during sexual contact can become a serious problem. Finally, this condition may cause erectile dysfunction due to psychological and anatomical reasons, especially if other reasons such as diabetes, atherosclerosis, use of sedatives and antihypertensives drugs or neurological diseases, preexist.
The diagnosis is easily accomplished by the medical history and the palpation of the plaque, and the penile ultrasound can verify possible calcification of the plaque. In cases of Peyronie’s disease with erectile dysfunction, a control of the blood supply of the penis by color Doppler could be performed to exclude dysfunction of the venoocclusive mechanism.
Various medications have been tried for conservative treatment of Peyronie’s disease, such as oral administration of vitamin E, paraminobenzoic acid (Potaba), colchicine and tamoxifen and injections of collagenase, corticosteroids and interferon in the fibrous plaque. Recently Xiaflex injections in the plaque given promissing results. The oral pharmaceutical treatment is usually not effective. However, since the surgical repair of the curvature is recomended after the resolution of the acute phase and the stabilization of the curvature, which usually takes at least six months after its appearance, the patient may try some medical treatment during this waiting period. Recently a combination of tadalafil 5mg once a day for six months with daily use of a penile strecher device have presented promissing results in penile straightening.
The most effective treatment for the repair of the curvature of the penis is surgery. There are three categories of surgical techniques to straight te penis. The selection of the method depends on anatomical parameters, that is the length of the erected penis and the degree of the curvature, the presence and the severity of a possible preexisting erectile dysfunction, the patient’s desire and the doctor’s experience.
The first category includes the techniques of shrinking of the corpora cavernosa in the oposite site of the curvature by sutures, with or without removal of “windows” of the fibrous sheath of the corpora (tunica albuguinea). This creates actually an opposite curvature, which counterbalances the existing curvature and thus the penis is straightened. The surgeon controls the repair of the curvature during the operation by causing artificial erections and may put more sutures until the desired result is achieved.
These techniques are effective, easy, fast, can be performed with spinal anesthesia and the duration of hospitalization is one day. They do not affect adversely the erections and also do not present serious complications. The patient can fully return to his activities after two or three days. He can have a sexual contact after a month. Many patients afraid, that with these techniques may have an additional loss of length of their penis, due to the shrinkage. However, this is not really the case, because the lost length is due to the curvature that was caused by their disease and not by the straightening operation.
The second category include techniques of complete removal or cutting out the Peyronie’s plaque and closing of the created gap of the fibrous sheath (tunica albuguinea) by an implant. Cutting out the plaque usually in the shape of an a H results to loosening of the corpora cavernosa during erection and consequently to straightening of the penis. This tecnique is easier than complete removal of the Peyronie’s plaque, with the same good results and fewer complications. Various implants are used to cover the gap of the tunica.
The problems with these implants, whether they become from the patient himself (autologous), like skin or venous implants collected from the legs, or from animals, like the bovine pericardium (heterologus), or are synthetic, are related with the significant prolonging of the operation, significantly higher cost and with the intervention of the surgeon andrologist on tissues he is not familiar with. A pioneering technique, that I have applied, is the coverage of the gap, after cutting out the plaque, by a free graft from the patient’s prepuce. The preputial graft is cheap, easy and fast to be collected, familiar to the urologist and without the disadvantages of the skin grafts like shrinkage and “ballon” formation on the graft site resulting to dysmorphia of the penis.
The main advantage of these techniques is that the penis is “unshrinking” during straightening, getting back its initial length. However, these operations are prolonged, expensive, relatively difficult, they require general anesthesia and hospitalization of three to four days. A circumcision is always performed. The sexual contact is allowed after one to two months. Complications, which may sometimes occur, include reduction of sensory of the glans and the appearance or deterioration of a preexisting erectile dysfunction. For these reasons, these operations are proposed only to patients with relative short penis, and/or big curvature more than 90 degrees or with a sandglass deformity of their penis. The use of a stretching device after the full healing can aid the full recovery of the length of the penis.
 Finally the third category of techniques are used in cases whith coexisting of severe erectile dysfunction and curvature. In these cases the placement of a penile prostheses with or without the application of appropriate mechanical handling of the plaque (modeling) during the implantation of the prostheses, repair both conditions with excellent results. There are no further problems regarding the function of the prostheses, due to the preexisting curvature, although sometimes the intense fibrosis, due to Peyronie’s disease, may makes the implantation difficult. However, in the hands of an experienced surgeon the results are always excellent.
Finally the third category of techniques are used in cases whith coexisting of severe erectile dysfunction and curvature. In these cases the placement of a penile prostheses with or without the application of appropriate mechanical handling of the plaque (modeling) during the implantation of the prostheses, repair both conditions with excellent results. There are no further problems regarding the function of the prostheses, due to the preexisting curvature, although sometimes the intense fibrosis, due to Peyronie’s disease, may makes the implantation difficult. However, in the hands of an experienced surgeon the results are always excellent.
Should the indications for the treatment of varicocele be widened?
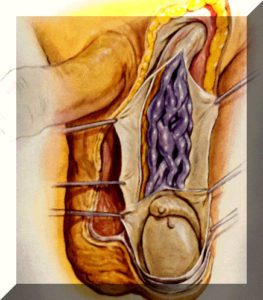
 A varicocele is a pathological cirsoid dilatation of the spermatic venous plexus of the testicle. It is due to a reflux of blood in the internal spermatic vein, which is the principal drainage vein of the testes, due to the insufficiency of valves that exist normally in the veins and allow the one-way blood flow towards the main vein that drains blood from the testicle, which is the renal vein. The insufficiency of these valves is usually congenital and the reflux of the blood increases with standing and severe fatigue, causing thus the dilatation of the veins.
A varicocele is a pathological cirsoid dilatation of the spermatic venous plexus of the testicle. It is due to a reflux of blood in the internal spermatic vein, which is the principal drainage vein of the testes, due to the insufficiency of valves that exist normally in the veins and allow the one-way blood flow towards the main vein that drains blood from the testicle, which is the renal vein. The insufficiency of these valves is usually congenital and the reflux of the blood increases with standing and severe fatigue, causing thus the dilatation of the veins.
The incidence of varicocele in the general population ranges between 4.4-22.6%; in subfertile men it ranges between 21-41% regarding primary infertility (that is when these men have no children at all) and 75-81% regarding secondary infertility. In the majority of cases (90%) the varicocele occurs on the left side, in 30-50% of the cases bilaterally and in 2% of the cases only on the right side.
The venous plexus, which exists around each testicle, as it has a winding form, acts as a heat exchanger with the environment, like the radiator of a car, so that the testicles can maintain a temperature that is at least one degree Celsius lower than the one of the abdomen. It is for this reason that the testicles are located outside the abdomen, in the scrotum. The formation of a varicocele, even in one testicle only, is harmful to this thermoregulatory mechanism, resulting to a sperm production disorder and therefore a fertility disorder. Furtermore, in patients with varicocele, due to the stasis of blood in the veins, free oxygen radicals are generated, which are particularly harmful to the sperm.
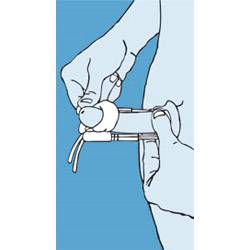
The diagnosis of varicocele takes place by the palpation of the dilated veins of the scrotum with the patient in standing position. In case of a varicocele of a small degree, where the veins are not easily palpable and visible, the patient is asked to strain himself with his mouth shut (the Valsalva maneuver), in order for the veins to fill with blood so that they can be palpable.
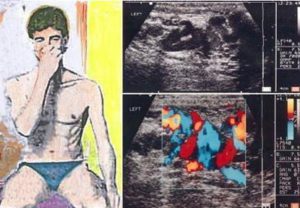
In the subclinical forms of the disease (non palpable even after the aforementioned maneuver), a diagnostic tool is the ultrasound of the scrotum and the color Doppler ultrasound (triplex). A dilatation of the spermatic veins which is greater than 3.5mm, with the simultaneous reversal of the venous flow during the Valsalva test, delimit the diagnosis. This examination must be also performed in the varicoceles that are palpable, so that the diagnosis can be verified.
The main indication regarding the treatment of varicocele is infertility. At this point the patients can feel a great anxiety and confusion for the following reason: The indication, which is set by the European and the American Association of Urology for the treatment of varicocele, regards men in couples that have not been able to have a child, despite their regular sexual intrecourses for a year and the man has a clinical (palpable) varicocele and an abnormal spermiogram.
However, even then, the couple should be aware that the fact that the possibility of having a child seems to increase, that does not mean that this couple will certainly have a child, which is of course what they desire, although the spermiogram has improved, which does not mean in its turn that it will certainly happen: all this does not mean that the treatment has not been properly performed. It is therefore obvious that, when the diagnosis of varicocele is made after a medical control which the patient desired to be performed, usually after a search on the Internet or the disorded has been diagnosed accidentally during a regular examination by a urologist, who was visited by the patient for some other reason, the question that arises is whether the disease should be immediately treated or not, as the issue of having a child has never been set forth.
A normal spermiogram somewhat reassures the patient, but the doubts if a disorder occurs in the future, or if there is a possibility, despite the normal spermiogram, that there is a difficulty in having a child in the future, exist as tormenting questions on the patient’s mind, and sometimes on the doctor’s mind, as they cannot be answered for the time being. All this occurs from the fact that the issue is having a child and nothing else.
Another important question, that occurs for varicocele is that, if the only treatment indication of varicocele is the one that has been mentioned and is included in the instructions of the European and the American Association of Urology or if there are indications that its treatment helps other fields. It seems that such indications indeed exist, and although they have not been yet adequately documented, so that they could be included in the instructions of the two scientific associations, the research towards this direction still goes on.
However, this documentation does not regard the safety of the treatment anyway, since its safety is granted, but only its effectiveness. Therefore, since the treatment of varicocele is simple, fast, easy, and without complications and without risk of relapsing, it could be applied in addition to the classical indication, in order to prevent or to improve the following conditions:
- Azoospermia
By this term we mean the absence of sperm in the semen, a diagnosis that can be made by a spermiogram. This condition is the only one that is related to the complete male infertility and, consequently, with the full incapacity to have a child in a normal way. All other sperm weaknesses, as they can be reflected in the spermiogram, do not exclude having a child in a normal way, they do just reduce the possibilities, depending on their gravity.
The prevailing opinion until today is that, since, in cases of azoospermia, the couple will either way follow the solution of in vitro fertilization, there is no need to treat a possible coexisting varicocele in the man. However, there is evidence today that the treatment of varicocele in the man before the in vitro fertilization increases the chance of finding sperm by a testicle biopsy, increases the pregnancy and birth rates and reduces the spontaneous abortion rates.
2. Progressive testicular damage
The far greater frequency of presence of varicocele in patients with secondary infertility, compared to the ones with primary infertility, supports the view of the progressive testicular damage. There are reports regarding the progressive worsening of the spermiogram image and of the testosterone levels in the blood of patients with varicocele, who have not undergone a surgical repair of the disease.
New data show that 87.5% of the patients with testicular dysfunction and 20% of nomospermic men with varicocele presented a progressive deterioration of the spermiogram, within a period of 63.2 months.
3. Pain
The effect of testicular pain in patients with varicocele ranges between 2-14%. Predisposing factors to the presence of testicular pain in patients with varicocele with a normal spermiogram are:
-the temperature of the scrotum
-the frequency of the reflux
-low body mass
-the distance of the renal sinus from the scrotum
It must be mentioned that the three last factors are statistically greater in patients with intense pain, than in patients with mild and moderate pain. The repair of the varicocele relieves testicular pain in 75% of the cases.
4. Reduction of the testosterone production
There are contradictory opinions regarding how much the repair of varicocele improves the production of testosterone in the testicles, which has already been reduced.
5. Damage to the genetic material (DNA) of the sperm
The damage to the DNA of the sperm is related with lower natural pregnancy rates, after artificial insemination, intracytoplastic sperm injection (ICSI) and classical in vitro fertilization (IVF).
The varicocele is related with a damage to the DNA of the sperm, which is possibly due to oxidative stress. The varicocele causes the generation of oxidative stress even in fertile men with normal sperm. Thus, it is well understood that there is a threshold of oxidative stress beyond which the fertility is affected. The repair of varicocele improves significantly the percentage of sperm with damage to its DNA.
6. Infertility in a normal couple
There are cases of couples with infertility, where the woman is perfectly normal and the man has a varicocele and his spermiograms are quite normal. In these cases, on the basis of what has been mentioned before, it is possible that the varicocele affets the microenvironment of the sperm, without altering the parameters of the spermiogram. Thus, its treatment could reverse these abnormalities and allow a pregnancy.
The treatment of varicocele is only surgical. There are various techniques with almost similar effectiveness. They all aim at stopping the abnormal reflux of blood to the venous network of the testicle, by interrupting the venous drainage of the organ by the ligature and incision of the internal spermatic vein and/or its branches. Attention must be paid to the fact that some of them are particularly overestimated (for example laparoscopic surgery), and they are not optimal regarding their advantages. The complications are either way minor in the hands of an experienced surgeon. The varicocele is not a relapsing disease. There may be a presence of dilated veins in the postoperative ultrasound, but this is not a sign of relapse or of an unsuccessful operation, because it is possible that there is no regression of the dilatation, but the reflux of the blood stops, which is the aim of the treatment. Respectively, the spermiogram needs 3 months after the operation in order to start improving, which improvement can continue for another 9 months. However, there is a chance that this does not happen, but this again does not mean that the operation has failed. Furthermore, even if the spermiogram does not improve, it is not impossible that a pregnancy is achieved.
Conclusions
The repair of the varicocele improves qualitatively and quantitatively the sperm, even in men over 40 years old and, the sooner it is treated, the better are the results. It inhibits the progressive deterioration of the sperm. It increases the chance of spontaneous pregnancy in patients with weak sperm, regarding the sperm count and/or motility. It increases the possibility of presence of sperm in the semen and the possibility of pregnancy in patients with azoospermia. It improves the outcomes of in vitro fertilization and reduces the rate of miscarriage after it. It increases the serum levels of testosterone, even in men over 40 years old. It eliminates or improves substantially a possible disturbing chronic testicular pain. Finally, it reduces the oxidating stress of the sperm and improves the percentage of the sperm with normal intact DNA, which is theoretically related with the improvement of fertility.
Consequently, given the fact that there is a low morbidity, a low rate of complications and a low cost, in contrast with the assisted reproduction method, particularly in couples where the woman also has infertility problems, should varicocele be operated more frequently than the classical indication of the European and the American Association of Urology?
